Welcome to the educational program Early Stages: Family Involvement and Planning. This program will present a brief overview of the changes associated with the various stages of Alzheimer’s disease. It will provide strategies for family involvement in caregiving and information about care planning.
. . .
This is Lesson 11 of The Alzheimer’s Caregiver. You may view the topics in order as presented, or click on any topic listed in the main menu to be taken to that section.
We hope that you enjoy this program and find it useful in helping both yourself and those you care for. There are no easy answers when it comes to the care of another, as every situation and person is different. In addition, every caregiver comes with different experiences, skills, and attitudes about caregiving. Our hope is to offer you useful information and guidelines for caring for someone with dementia, but these guidelines will need to be adjusted to suit your own individual needs. Remember that your life experiences, your compassion and your inventiveness will go a long way toward enabling you to provide quality care.
Let’s get started.
Alzheimer’s Disease
Alzheimer’s disease is a type of dementia characterized by a progressive loss of cognitive, or mental functioning. It commonly occurs in the later years of life, though its cause is still unclear.
Alzheimer’s disease causes damage and eventual death to nerve pathways and cells. These losses prevent the brain from being able to function normally. This includes changes in the brain’s chemistry and structure, and the loss of the brain’s ability to process information.
 Alzheimer’s disease also causes damage to brain cells, which eventually die. These cells are important because they process and store information and generate ideas. The brain pathways that send messages about seeing and hearing, movement, emotions, and thoughts are also eventually lost.
Alzheimer’s disease also causes damage to brain cells, which eventually die. These cells are important because they process and store information and generate ideas. The brain pathways that send messages about seeing and hearing, movement, emotions, and thoughts are also eventually lost.
In addition, Alzheimer’s often first affects the cells in the hippocampus, a center in the interior of the brain that processes and stores all new information. This is why in Alzheimer’s disease, recent memory is affected early on.
These losses not only affect the brain, but affect a person’s behavior, personality and their overall ability to function properly. For example, activities of daily living such as eating, bathing and dressing become too difficult for the person to perform without the assistance of a caregiver.
Changes in Behavior
Let’s look at some of the ways that Alzheimer’s causes changes in behavior and personality. One way is, an affected individual may become suspicious and mistrusting of other people, or seem overly concerned and secretive about money and other valuables.
This paranoia and suspiciousness can develop because of misperceptions, causing the person to be secretive and uncooperative, even hostile toward persons trying to help.
Individuals may also wander as though they are looking for something, or appear depressed or uninterested in their environment.
What previously may have been considered minor concerns may now cause great irritation or even anger and aggression. Wandering, pacing, restlessness, and catastrophic or explosive reactions are commonly seen in people with Alzheimer’s disease and may reflect different manifestations of agitation. This verbal and sometimes physical aggression are common reasons for placement in a care facility.
Apathy or lack of motivation is a symptom of the disease and may be the initial clue that something is wrong. A successful businessman, for example, may lose his job for lack of initiative or low productivity. Apathy is often confused with depression and can contribute to immobility, malnourishment, poor dental hygiene and many other debilitating situations.
Challenging behaviors may worsen and cause excessive stress and anxiety for the caregivers, interrupting their sleep and affecting their health. Tension can escalate in these circumstances and may lead to care recipient abuse.
Misperceptions
 People with Alzheimer’s can also suffer from misperceptions, including delusions, illusions and hallucinations.
People with Alzheimer’s can also suffer from misperceptions, including delusions, illusions and hallucinations.
Delusions are strongly held ideas or beliefs that have no basis in reality, while illusions are misperceptions or misinterpretations of real objects in the environment. An example of an illusion is mistaking a hat rack for a person or mistaking a shadow for a pet dog.
Hallucinations are perceptions of things that are not there, such as hearing music when there is none, or seeing ants in the bed when there are none. These false perceptions are related to chemical and physical changes in the brain that alter the ability to accurately process information in the environment.
Changes in Abilities
Those with Alzheimer’s disease also experience changes in functional abilities. They may increasingly get lost, lose  things, forget to pay bills, neglect hygiene, dress and groom poorly, and have difficulty communicating their needs.
things, forget to pay bills, neglect hygiene, dress and groom poorly, and have difficulty communicating their needs.
These functional losses can be categorized as amnesia or losses in memory function; aphasia or difficulty speaking and understanding language; agnosia, problems recognizing people, objects and places; and apraxia, a loss of the ability to perform every day activities such as dressing, brushing teeth or combing hair.
Stages of Alzheimer’s Disease
An important aspect of Alzheimer’s disease is that these changes do not appear all at once. Alzheimer’s is a progressive  illness that can last 8 to 20 years, with changes occurring gradually over months and years. Because it is a progressive illness, changes, care issues and management planning, are often considered in terms of the “stages of the illness”. The most common classification of stages and the one that we will use, is simply using the terms: early, middle, late and end stage.
illness that can last 8 to 20 years, with changes occurring gradually over months and years. Because it is a progressive illness, changes, care issues and management planning, are often considered in terms of the “stages of the illness”. The most common classification of stages and the one that we will use, is simply using the terms: early, middle, late and end stage.
As we discuss the “stages” of Alzheimer’s disease and other forms of dementia, it is important to keep in mind that these are only general categories or phases that serve as guidelines in understanding and planning care. Our brains, our bodies and our personalities are very different and we will all manifest an illness, even a brain disease, differently.
Keeping that in mind, here is a general outline of behaviors and functions in the various stages of Alzheimer’s disease.
Stages of Alzheimer’s disease (Continued)
In the early stage of Alzheimer’s disease, the changes can be very subtle and attributed to aging. People begin to forget appointments, names, and places. They may lose valuable items and suspect others of stealing, so they may begin hiding things only to forget where they’ve been hidden. People may also become obsessed with certain persons, valuable items or events as an effort to maintain contact with or control of them. Individuals may be restless or depressed and  apathetic. Sleep disturbances can occur in the early stages and worsen as the disease progresses. People often lose social graces, but because they may otherwise function well, these problems may be attributed to stress, illness or fatigue. However, once a diagnosis has been made, people often look back and see some behaviors or difficulties that were part of the disease process. In the early stage, affected individuals will have some awareness of the situation and may share their concerns with a spouse or adult child and ask questions about what it means for them and their family. It is best to treat these concerns with honesty.
apathetic. Sleep disturbances can occur in the early stages and worsen as the disease progresses. People often lose social graces, but because they may otherwise function well, these problems may be attributed to stress, illness or fatigue. However, once a diagnosis has been made, people often look back and see some behaviors or difficulties that were part of the disease process. In the early stage, affected individuals will have some awareness of the situation and may share their concerns with a spouse or adult child and ask questions about what it means for them and their family. It is best to treat these concerns with honesty.
In the middle stages, people will have difficulty with managing money, legal affairs, workplace duties, driving, and functioning in new environments. Home maintenance, housekeeping and cooking will become more challenging. In this stage, personality changes become evident. Difficult behaviors and sleep pattern changes may also become more common.
In the late stages, people will have increasing difficulty with activities of daily living, such as bathing, grooming, toileting, and mobility. They will show frustration, agitation, and have language difficulties. There is usually greater disturbance of sleep patterns, including nighttime wakening and sleeping during the day. In the end-stage of Alzheimer’s disease, people are no longer able to walk or recognize family members. They will lose weight, become incontinent and will need complete care. However, remarkably, many in this end stage of the disease will have moments of recognition and better understanding of language.
Planning Care
 Planning the care of someone with dementia can seem overwhelming. One of the first things to do after a family member has been diagnosed with Alzheimer’s disease is to make sure that all family members are informed and involved in the planning process. The primary caregiver and other family members should educate themselves, obtain information about the disease, and locate and investigate what resources are available.
Planning the care of someone with dementia can seem overwhelming. One of the first things to do after a family member has been diagnosed with Alzheimer’s disease is to make sure that all family members are informed and involved in the planning process. The primary caregiver and other family members should educate themselves, obtain information about the disease, and locate and investigate what resources are available.
Educational Materials
 Though informing yourself on the disease will help you in the caregiving process, it will by no means make it easy, as the task of caring for people with dementia is always a difficult one for everyone involved. There will be stress and emotional reactions.
Though informing yourself on the disease will help you in the caregiving process, it will by no means make it easy, as the task of caring for people with dementia is always a difficult one for everyone involved. There will be stress and emotional reactions.
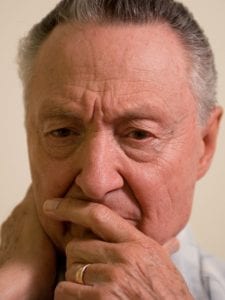
It is especially difficult for adult children to see their once strong, independent father or mother, whom they looked up to for so many years, a shadow of their former selves. This recognition is also painful for any individual who knew the person before the disease.
Due to the burden and stress of caregiving, caregivers may suffer from their own declining health during this protracted illness.
Involving Family Members

After diagnosis, it is essential that family members be involved in planning for the person’s care. In most cases, the changes associated with Alzheimer’s disease will happen gradually, so early planning can be more general in nature, leaving the details to be explored as the need arises.
From very early on, it is essential that all family members participate in some way in the day to day care of the individual. This will help to support the primary caregiver by giving them some respite. Because Alzheimer’s care is a long-term commitment, it is important for primary caregivers to take the time to take care of their own mental and physical health and maintain social contacts. Having family come to help provide care also gives adult children and siblings an understanding of the illness and the role of caregiving. Caregiving is also an opportunity to contribute in the care and support family solidarity.
Family members can also help to monitor the symptoms as the disease progresses, as they may notice things that the primary caregiver does not. If symptoms increase in frequency or severity, it is important to share this with other family members and the person’s healthcare providers.
Of course, some family members may live far from the affected individual and will not be able to provide hands-on assistance on a regular basis. These relatives should never-the-less be considered part of the care team. They need to be consulted and included in decisions when possible. This can be done through regularly scheduled telephone communication and occasional visits to the person, which are beneficial for everyone involved.
Investigate Resources
 Early in the course of the illness, families need to learn about information resources and alternative care possibilities. Though perhaps not required initially or at all, families should at least be informed about alternative care resources such as in-home assistance, day care, residential and hospice care. Emergency services including the Alzheimer’s Association “Safe Return” program should also be investigated. The Safe Return program is discussed in more detail in another section.
Early in the course of the illness, families need to learn about information resources and alternative care possibilities. Though perhaps not required initially or at all, families should at least be informed about alternative care resources such as in-home assistance, day care, residential and hospice care. Emergency services including the Alzheimer’s Association “Safe Return” program should also be investigated. The Safe Return program is discussed in more detail in another section.
ARARF Website
 As you know, one information resource is Alzheimer’s Research and Resource Foundation. The ARARF website provides valuable information about Alzheimer’s disease and other types of dementia, many of which are free. There are educational materials on numerous topics including communication, mealtime management, sleep, behavior issues, activities, incontinence, bathing, dressing and grooming.
As you know, one information resource is Alzheimer’s Research and Resource Foundation. The ARARF website provides valuable information about Alzheimer’s disease and other types of dementia, many of which are free. There are educational materials on numerous topics including communication, mealtime management, sleep, behavior issues, activities, incontinence, bathing, dressing and grooming.
You can also find more information via the Alzheimer’s Association and the U.S. National Institute of Health’s Alzheimer’s Disease Education and Referral Center (ADEAR).
Alternative Care Resources
Given the research, we emphasize home care in this program and believe that, when possible, it is the most beneficial setting for someone with Alzheimer’s disease. However, it is a good idea for families to know about alternative care resources in advance of needing them.
 The idea of a “continuum of care” has long been a way of planning for the care of people as their health conditions improve or decline. For example, a person who has had a heart attack will need close medical and nursing care for a period of time, including hospitalization. As treatment is provided and the condition improves, less intense care is needed . The person can then continue care at home or a rehabilitation care facility.
The idea of a “continuum of care” has long been a way of planning for the care of people as their health conditions improve or decline. For example, a person who has had a heart attack will need close medical and nursing care for a period of time, including hospitalization. As treatment is provided and the condition improves, less intense care is needed . The person can then continue care at home or a rehabilitation care facility.
On the other hand, some conditions and diseases have progressive courses, such as Parkinson’s and Alzheimer’s disease. So the care needs continue to increase rather than decrease.
Case Study 1
 Here is a case study in which complimenting home care may be considered.
Here is a case study in which complimenting home care may be considered.
Mary cares for her husband, Robert, who has Alzheimer’s disease, at home. She is 60 years old and he is 70. Mary has been able to manage his care in their home for the 2 years since his diagnosis. She cooks his meals and sits to eat with him. She helps him into the shower to bathe and lays out his clothes so that he can dress himself. Mary was recently seen by her physician for dizziness, and her blood pressure was reported to be 164/90. The doctor prescribed diet, exercise and medication, and advised her to ‘take it easy’ and avoid stress.
What is the best solution for Mary and Robert in this situation?
- A. Enroll Robert in an adult day care program for 2 to 5 days a week.
- B. Get home care assistance.
- C. Continue caregiving by herself.
Case Study 1 Answers:
Choice A: “Enroll Robert in an adult day care program for 2 to 5 days a week” is a good answer.
Enrolling your loved one in a “Day care” program could be very beneficial. Adult day care is a site away from home that provides daytime care for elders and respite for family caregivers. Programs vary widely, but generally provide socialization, physical exercise, mental stimulation, nutritious meals, and most will provide transportation to and from the center.
The stimulation provided in Adult Day Care for people with Alzheimer’s disease can improve alertness and general function. This could be beneficial for Robert and allow Mary to pursue the doctor’s advice for exercise, rest, and less stress.
Choice B: “Get home care assistance” is also a good choice.
In-home assistance can be helpful when the family prefers to care for a person at home but the primary caregiver needs some help with caregiving.
In Mary’s case, simply having someone come to the home a few times per week, or more often when needed, will relieve some of his caregiving burden. Home care assistance can help prepare meals, clean the home, wash laundry and dishes, help deal with issues, and provide transport to places.
Choice C: “Continue caregiving by herself” is not a good choice.
Mary has high blood pressure and has been prescribed medication and an exercise and diet regime. If she is going to be able to provide care for Robert, she needs to take care of herself as well. She needs to take time away from caregiving to attend to her own health. If something should happen to her, who would take care of Robert?
Continuum of Care
 The idea of a continuum of care is that planning begins early in the disease process. Though caregivers may wish to provide all of the care by themselves, they need to recognize that the illness progresses and that caregiving demands and the associated stress increase. The goal is for the caregiver to transition from being the sole caregiver to having assistance in the home and to accessing a day care program. The nature of the illness is that there will be a need for a more intense level of care over the years, so knowing what the resources are and when and how to access them is essential.
The idea of a continuum of care is that planning begins early in the disease process. Though caregivers may wish to provide all of the care by themselves, they need to recognize that the illness progresses and that caregiving demands and the associated stress increase. The goal is for the caregiver to transition from being the sole caregiver to having assistance in the home and to accessing a day care program. The nature of the illness is that there will be a need for a more intense level of care over the years, so knowing what the resources are and when and how to access them is essential.
The important thing to remember is that Alzheimer’s disease has a long course and requires an increasing amount of care. Caregivers need to care for themselves, involve other family members, accept help, and plan for the long-term needs of their loved one and for themselves.
Continuum of Care (continued)
As a general rule, the longer an individual can remain in the familiar environment of their own home, the better their  adjustment will be to subsequent levels of care, including day care and 24 hour residential care.
adjustment will be to subsequent levels of care, including day care and 24 hour residential care.
There are a number of resources that provide assistance with home caregiving. Among these are nutrition programs such as “Meals on Wheels”, congregate meals, Senior Companions, respite care, support groups, and volunteers.
Nutrition Programs
 In “Meals on Wheels”, volunteers from the state centers on aging deliver hot meals to home-bound individuals on a daily basis. Volunteers are trained, not only in the nutritional and distribution components of the program, but in visitation aspects of the service as well. Information on obtaining this service can be found in your local phone directory or on the internet under state or local offices on aging or senior services.
In “Meals on Wheels”, volunteers from the state centers on aging deliver hot meals to home-bound individuals on a daily basis. Volunteers are trained, not only in the nutritional and distribution components of the program, but in visitation aspects of the service as well. Information on obtaining this service can be found in your local phone directory or on the internet under state or local offices on aging or senior services.
Caregiver Support
 Respite care services are available through most Alzheimer’s Association Chapter offices. Respite care can take the form of a volunteer from the Alzheimer’s Association who has been trained in Alzheimer caregiving. These are often individuals who have been caregivers for a member of their own family.
Respite care services are available through most Alzheimer’s Association Chapter offices. Respite care can take the form of a volunteer from the Alzheimer’s Association who has been trained in Alzheimer caregiving. These are often individuals who have been caregivers for a member of their own family.
Some Alzheimer’s Association chapters have a separate fund for helping families pay for an aide or temporary “sitter” for a limited number of hours per week. Overnight respite services can be provided by 24 hour Alzheimer’s care facilities when a primary caregiver needs to be away for a period of time. These can be found in the local phone book or through the Internet. A local Alzheimer‘s Association chapter will have lists of many types of respite services.
Support Groups
 Caregiver support groups can provide a forum for support and the exchange of ideas about caring for a loved one. Caregivers can find comfort in the support from others with similar difficult and painful experiences.
Caregiver support groups can provide a forum for support and the exchange of ideas about caring for a loved one. Caregivers can find comfort in the support from others with similar difficult and painful experiences.
Most caregivers will be able to find support groups in their own communities. In some cities, there are support groups for different stages of the illness. There may also be some meetings where both the caregiver and the person with dementia attend together.
Information about support groups in your community can be obtained through local or state Alzheimer’s Associations.
The helpline, available 24 hours/7 days per week is 1-800-272-3900, and more information can be found here: http://www.alz.org/index.asp.
Volunteers
 Caregivers may also find support and assistance from a church or temple, as some religious organizations have outreach programs for their members and even non-members in need. For information about this, you should contact your local religious organizations.
Caregivers may also find support and assistance from a church or temple, as some religious organizations have outreach programs for their members and even non-members in need. For information about this, you should contact your local religious organizations.
Safe Return® Program
Because of the decline in the ability to recognize their surroundings, those with dementia may wander away from home and find themselves in great danger from street traffic, severe weather, or dangerous neighborhoods. Caregivers should  consider registering their loved one in the Alzheimer’s Association’s Safe Return™ program.
consider registering their loved one in the Alzheimer’s Association’s Safe Return™ program.
This is a nationwide identification, support and enrollment program that provides assistance when a person with Alzheimer’s disease or a related dementia, wanders and becomes lost. Assistance is available 24 hours a day, seven days a week.
If a person is missing, a phone call to Safe Return activates a community support network to help reunite the lost person with the caregiver. Safe Return faxes the enrolled person’s information and photo to local law enforcement. When the person is found, Safe Return notifies listed contacts. The nearest Alzheimer’s Association office provides information and support during the search and rescue efforts.
For more information on the Safe Return Program, click on the provided link.
Click here to learn about the Safe Return® program.
Congregate Meals
 Congregate meals are provided in local Senior Centers and offer an opportunity for socialization as well as nutrition. Nutritious meals are prepared in a central location and delivered to the senior centers or other congregate site. The cost for the meal is minimal and some free meals may be available, depending on the situation. For those who are not able to drive or walk to the senior center, transportation can often be arranged.
Congregate meals are provided in local Senior Centers and offer an opportunity for socialization as well as nutrition. Nutritious meals are prepared in a central location and delivered to the senior centers or other congregate site. The cost for the meal is minimal and some free meals may be available, depending on the situation. For those who are not able to drive or walk to the senior center, transportation can often be arranged.
To learn more about nutrition programs: Meals on Wheels www.Mowaa.org Tel: 703.548.5558 AoA info on congregate meals: www.AoA.gov
Senior Companions
 Senior Companions is a program under the National Senior Service Corps. This is a network of federally supported programs that provide opportunities for seniors to volunteer their time as Foster Grandparents, Senior Companions, and Retired Senior Volunteers.
Senior Companions is a program under the National Senior Service Corps. This is a network of federally supported programs that provide opportunities for seniors to volunteer their time as Foster Grandparents, Senior Companions, and Retired Senior Volunteers. The Senior Companion program is part of the Corps. Interested seniors are recruited and trained to provide visitation in homes for home-bound elders. The purpose of the visitation is to provide mental and social stimulation and loving attention.
Click here to learn more about Senior Companions
Hospice Care
 During the end stage of Alzheimer’s disease, some caregivers consider hospice care.
During the end stage of Alzheimer’s disease, some caregivers consider hospice care.
Hospice care is a service for individuals who are nearing the end of their lives that can be provided in the home, residential facility, hospital, or professional hospice facility. The goal of hospice care is to provide people with support and comfort by relieving pain and other symptoms so that their last days may be spent with dignity surrounded by their loved ones. The focus of hospice is caring, not curing, and to provide the highest quality of life during whatever time remains. Hospice care does not hasten or postpone death.
Individuals with Alzheimer’s disease are eligible for this service, which is generally paid for by Medicare, and in some states, Medicaid.
Summary
In summary, it is important to involve all family members in the care of someone with Alzheimer’s disease. All family members should learn about the disease, how to care for someone with it, and what resources are available to help them through the months and years to come. They also need to become involved with caregiving in an active way, recognizing that the primary caregiver will have a heavy burden, even in the early stages, and most certainly as the disease progresses.
Some of the available resources and services include respite care services, nutrition programs such as Meals on Wheels, volunteer programs such as Senior Companions, Support groups, the Alzheimer’s Association, and hospice care
← Previous Lesson (Managing Difficult Behaviors)
→ Next Lesson (Early Stages at Home: Intimacy and Sexuality)
. . .
Written by: Catherine M. Harris, PhD, RNCS (University of New Mexico College of Nursing)
Edited by: Mindy Kim-Miller, MD, PhD (University of Chicago School of Medicine)
References:
- Assisted Living Federation of America. (2008). Federal statutes that impact assisted living. Retrieved on February 10, 2009 from http://www.alfa.org/i4a/pages/Index/
- Butcher HK, Holkup PA, Maas M, (2001). Thematic analysis of the experience of making a decision place a family member with Alzheimer’s disease. Res Nurs Health 24(6): 470-80.
- Calkins MP & Namazi KH. (1991). Caregivers perceptions of the effectiveness of home modifications for community living adults with dementia. Journal of Alzheimer’s Care and Related Disorder Research, 6:1:25-29.
- McClendon MJ, Smyth KA, Neundorfer MM, (2006). Long-term-care placement and survival of persons with Alzheimer’s disease. Journals of Gerontology Series B. 61B(4) p220-7.
- Gaugler J, Leach C, Clay T, Newcomer R, (2004). Predictors of nursing home placement in African Americans with dementia. Journal American Geriatrics Society 52:445-452.
- Gerdner LA, Hall GR, (2001).Chronic confusion. In ML Maas, KC Buckwalter, MD Hardy, T Tripp-Reimer, MG Titler, & JP Specht (Eds), Nursing care of older adults: Diagnoses, outcomes, & Interventions.(pp. 421-441). St. Louis. Mosby.
- Home safety for people with Alzheimer’s disease. (2007). Alzheimer’s Disease Education and Referral. National Institute on Aging, NIH Publication.
- McClendon MJ, Smyth KA, Neundorfer MM, (2006). Long-term-care placement and survival of persons with Alzheimer’s disease. Journals of Gerontology Series B. 61B(4) p220-7.
- Schur D, Whitlach CJ, (2003). Circumstances leading to placement: A difficult caregiving decision. Lippencott’s Case Management 8 (5): 187-97.
- Warner M & Warner E (1996). The caregiver’s guide to home modification. In M L Warner: The complete guide to Alzheimer’s proofing your home. Purdue University Press.
- Wang S, Davies E, (2007). Journal of Nursing (China). Jun; 54(3): 82-86.